
|
Joeri van Ormondt, MSc, SLT, CESS-certified stuttering specialist from The Netherlands, owns private practice De Stotterpraktijk, specialised in stuttering and cluttering. He is a person who stutters, RESTART-DCM-trainer, CESS-board member and ESS-teacher/coach. He co-founded Stotterconnect, an organization dedicated to Camp Dream. Speak. Live. and the training of SLT’s.
|



When a young child begins to stutter, it can be a challenge for the child, their parents, or both. When faced with such a challenge, people often turn to therapy, hoping it will ease the difficulty. Put simply, therapists see two groups: one in which stuttering continues, and another in which it fades away. How can we optimize early stuttering therapy to meet the needs of both groups? In this article, we argue for a reset of the general approach to stuttering in children under six. If we shift our focus in early stuttering therapy, it can build strength and reduce stigmatization from the very moment stuttering appears.
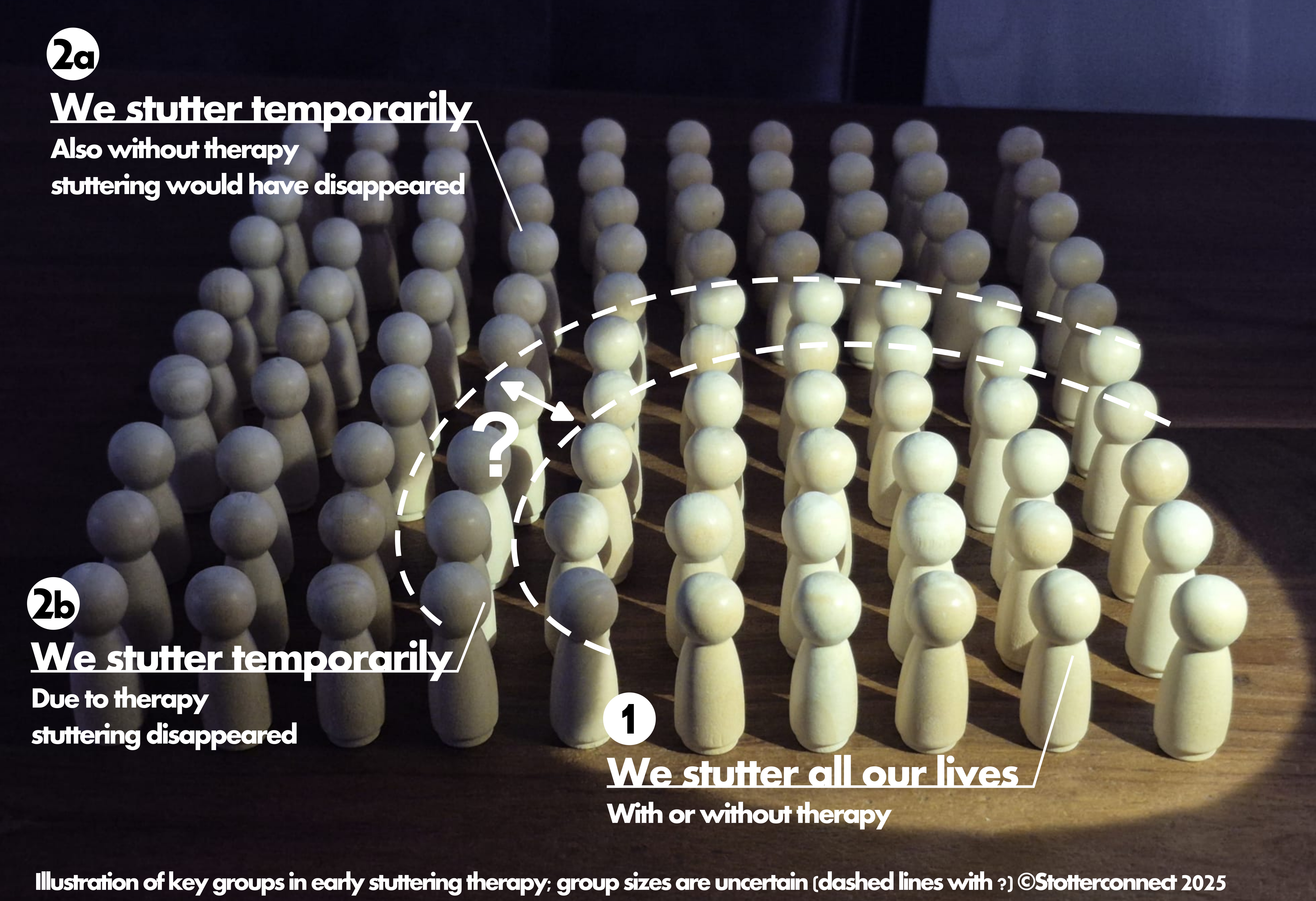
Traditionally, therapy has aimed to reduce or eliminate stuttering. In early stuttering therapy, measuring the effectiveness of therapy with this outcome has been a persistent challenge for decades. Exact figures are hard to establish,[3, 8] -as percentages vary across studies- but a visual impression helps convey the general picture (see figure). One group of children will continue to stutter throughout life, even after early childhood therapy (group 1). The other group consists mostly of children whose stuttering would have disappeared without therapy (group 2a), and of children for whom therapy may have contributed to the fading of stuttering (group 2b).
While research on possible negative side effects of early therapy programs in the long term -so for group 1- is lacking, evidence is growing that efforts to minimize stuttering may harm children’s self-confidence and development later in life. Many adults who stutter say they wish stuttering had truly been accepted as okay when they were young[1, 2, 4] . Children who stutter also face stigma in a society that largely views stuttering as a problem to be solved, a view likely reinforced by the common belief that therapy exists to eliminate stuttering. We believe the general public overestimates the size of group 2b, which is understandable, since many in group 2a also believe they no longer stutter only because of therapy – and in doing so, unintentionally contribute to that stigma.
We still don’t know what the working ingredient is in early childhood stuttering programs that aim to reduce overt stuttering[7]. What we do know is that growing up with a stutter puts these children at risk of developing negative beliefs about their speech and themselves. We also know how to reduce this impact of stuttering. So let’s look at the commonly used general approach and its consequences.
We once worked with the traditional focus. Together with parents, we made a therapy plan with reduction of stuttering as the primary outcome, presumably leading to the child’s stuttering to disappear. We made parents aware of the ‘window of opportunity’ and therapy was viewed as a last chance to benefit from it. For both parents and therapists, success meant being able to say the child no longer stuttered.
As mentioned before, stuttering did not always fade (group 1) during therapy. From the start, we included a disclaimer, telling parents about this group who would continue stuttering. For every child in group 1 after a year or more, therapy did not achieve its main goal. We then shifted focus to a different outcome: reducing the impact of stuttering. The shift to this ‘second-best’ outcome implies failure, possibly reinforcing the idea that stuttering is undesirable. As a result, negative beliefs and attitudes -the stuttering iceberg- may have grown already. And note, there has -as far as we know- never been a study on harmful side effects of therapy.
In the past decade, there have been ongoing discussions, alongside a shift in our field, toward neurodiversity and stuttering-affirming therapies. Young children’s therapy was largely left out of these discussions. We therefore call for a critical evaluation of therapy for children under six. What if we turned therapy around and affirmed stuttering in all children? When a child begins to stutter, we do not know to which group the child will ultimately belong.Therefore, let us consider as if all children belong in group 1 from the very beginning. Because for children that are in group 1 it is crucial to give them -right from the first session- the strengths they need. No growing iceberg. No undoing of earlier therapy. Accepting parents. Strong children. We strongly believe this shift of focus benefits all children without the side effects mentioned above. This is why we believe early therapy remains vital. Below, we outline some key considerations for this paradigm shift[2]: rephasing therapy goals, changing language and helping children and parents feel relaxed about stuttering.
The first change we suggest is rephrasing the goal of therapy into one that is realistic and accessible for all children. For these children, the aim is to enjoy communication, speak freely, or communicate effectively. These objectives give parents and children the satisfaction of working toward something they can influence. So, no goal focused on stuttering reduction.
Changing the language around stuttering is another key factor to be considered[5]. This runs throughout therapy. Languagestems from how we view stuttering. If you see stuttering as a disorder, you will use different language than if you see it as a human difference; a variation in speaking or a communication difference. This matters: the framework shapes the language we use. For example, it is still common -especially with this age group- to speak of recovery from stuttering. Yet recovery, like terms such as risk factors and stuttering severity, is mainly associated with disease. Much medical-model language remains embedded in our thinking. Because it was once so widespread, we may not even notice when we use it. However, it is just a word you use. And words can be replaced; doing so can greatly influence how parents view stuttering and their child. By modeling, explaining, and rephrasing language, we help parents build the strength in their child to foster confident, strong communication.
We think therapy is unlikely to be effective while environmental pressure to cure stuttering persists. We therefore see it as crucial to help parents and children feel relaxed about stuttering. Any form of pressure shapes the communication style modeled for the child. We illustrate this with some examples.
A four-year-old girl showed many secondary behaviors, which stressed her mother considerably. It did not matter what approach we used, the girl’s secondary behaviors and frustration did not change. Attending therapy itself created a constant urge in the mother to eliminate stuttering, so her daughter wouldn’t face negative experiences later in life. In the end, what proved effective was fully letting go of therapy. This allowed the mother to release her focus on controlling stuttering, leading to more relaxed communication for both mother and child.
Recently we saw another child, three years of age. Therapy had not yet begun when the parents, calling from their holiday, panicked because stuttering had increased significantly. We taught the parents how to talk about stuttering with their son. A few days later, the parents heard him tell the neighbors that he stutters – and that it’s okay. He still stuttered, of course, but secondary behaviors decreased significantly. Communication became fun and easy again. And importantly, the parents were at ease.
In general, we see parents value such openness about stuttering greatly. Their child acquires useful tools to be independent in future situations and to build strengths. This gives parents confidence their child can handle questions or ‘jokes’ about their speech. It greatly reduces parents’ worries. This also works with younger children. We have seen it time and time again. The above examples show why early therapy with parents and children is vital, with reducing stress around stuttering as the first step. This means talking and learning about stuttering, exploring it, and making room for the emotions of both children and parents. A next step in therapy can be easing communicative pressure (for example, turn-taking behavior, reducing questions asked by parents, and adjusting language to the children’s needs). We make communication fun (again) and give the children the best opportunities to express themselves with strength and ease.
Since we started reframing our thinking and language about stuttering to be more inclusive and (neuro)diversity-affirming, something interesting happened. Parents and children seem far more relaxed about stuttering. For most parents, it no longer matters whether a child continues to stutter, because they have the strengths to keep the iceberg from growing. We believe this attitude makes therapy far more effective and shorter.
We invite fellow professionals to reflect on their own work and, regardless of the program or components used, critically reconsider elements that focus mainly on reducing stuttering and may unintentionally raise communicative tension or reinforce stigma.
Finally, what about children whose stuttering will fade eventually (group 2)? It does no harm to approach them as children who stutter. After all, during therapy they are children who stutter. During their life, stuttering may come and go. That’s all okay. Imagine that a sibling of a child who used to stutter begins to stutter at some point. How powerful would it be if not only parents but also the older sibling – though no longer stuttering- knows everything about stuttering and can advocate for their younger sibling. Or to support others who stutter whom they encounter later in life. Or even themselves if their own stuttering returns. Therapy with this new focus will give the diverse stuttering community true strengths.
References
- Byrd, C., O’Dwyer, M., & Eggers, K. (2022). Building resilience through Camp Dream. Speak. Live. In K. Eggers & M. Leahy (Eds.), Clinical cases in fluency disorders (pp. 44–54). Routledge. https://doi.org/10.4324/9781003179016-5
- Byrd, C. T., Coalson, G. A., & Conture, E. G. (2024). CARE model of treatment for stuttering: Theory, assumptions, and preliminary findings. Frontiers in Psychology, 15, 1488328. https://doi.org/10.3389/fpsyg.2024.1488328
- Carey, B., Onslow, M., & O’Brian, S. (2021). Natural recovery from stuttering for a clinical cohort of pre-school children who received no treatment. International Journal of Speech-Language Pathology, 23(1), 48–56. https://doi.org/10.1080/17549507.2020.1746399
- Gerlach-Houck, H., Kubart, K., & Cage, E. (2023). Concealing stuttering at school: “When you can’t fix it… the only alternative is to hide it.” Language, Speech, and Hearing Services in Schools, 54(1), 96–113. https://doi.org/10.1044/2022_LSHSS-22-00029
- Lamoureux, G., Tessier, A., Finlay, S., & Verduyckt, I. (2024). Critical perspectives in speech-language therapy: Towards inclusive and empowering language practices. Disabilities, 4(4), 1006–1018. https://doi.org/10.3390/disabilities4040062
- Phillips, M. C., & Spaulding, T. J. (2025). Listening to voices that matter: The speech therapy experiences of people who stutter. Journal of Speech, Language, and Hearing Research. Advance online publication, 1–28. https://doi.org/10.1044/2025_JSLHR-24-00792
- Sjøstrand, Å., Næss, K.-A. B., Melle, A. H., Hoff, K., Hansen, E. H., & Guttormsen, L. S. (2024). Treatment for stuttering in preschool-age children: A qualitative document analysis of treatment programs. Journal of Speech, Language, and Hearing Research, 67(4), 1020–1041. https://doi.org/10.1044/2024_JSLHR-23-00463
- Yairi, E., & Ambrose, N. G. (2013). Epidemiology of stuttering: 21st century advances. Journal of Fluency Disorders, 38(2), 66–87. https://doi.org/10.1016/j.jfludis.2012.11.002
![]()
Hello Joeri, Femke, and Tjitske
Thank for your very interesting paper. I believe, too, that this is an important paper, in that it is, in my view, critically important for therapy for young children who stutter to be stuttering-affirmative, that is, to consider the stuttering – just as you wrote – as a difference, not a defect.
When dealing with a pre-school child who stutters, you have no way of knowing if they belong in group 1, 2a, or 2b. You have to treat every child the same, you have to assume that the stuttering will persist, and therefore provide the child and the parents with all the information and tools that they need to foster resilience and self-advocacy. You have to educate them all about stuttering – why we stutter, difference between stuttering and struggle – and, as you write, show them all that effective communication is not related to fluency.
I understand that this is exactly what you suggest, and how you approach therapy that you provide. For that, I am very thankful and grateful to you.
You write that “As mentioned before, stuttering did not always fade (group 1) during therapy. From the start, we included a disclaimer, telling parents about this group who would continue stuttering. For every child in group 1 after a year or more, therapy did not achieve its main goal. ” I suggest that there are cases where the therapeutic approach is defective, that the attitude of the therapist is defective (focus on fluency), and that these approaches cause much suffering. So, it is not sufficient to state that “stuttering did not always fade during therapy”. While that is true, perhaps it is sometimes the very attitude of the therapist that is the problem.
We should note that we do not yet know why stuttering fades in about 75% of the pre-school CWS. It fades with or without therapy, from what I understand. Please correct me if I am wrong. And so, treat every case as if the child will continue to stutter. The parents have to be taught to accept and embrace the stuttering, and not to cling to false hope that the stuttering will fade.
Once again, well done to you all for this excellent paper, and well done for improving approaches to therapy. You folks are amazing.
Hanan
Dear Hanan,
Thank you so much for your kind words. You are totally right 2nd and 3rd paragraph, that is what we suggest.
I agree with you that for a lot of children (but not necessarily for all) a stutter affirming attitude in therapy right from the start will help the child the rest of their life (regardless of the stuttering fades away after a while).
And no, we don’t know if stuttering will fade in a specific child. There are, though, some factors we can look at that give fading out a higher or lower probability. For example the most obvious one: if it is a girl it is more likely. But even with all ‘prediction’-boxes ticked, you are far from certain.
Thanks for your kind words!
All the best,
Joeri
I have worked intensively with stuttering (from 1971 until about ten years ago). Preventing stuttering from developing into a lifelong problem in children is the most important thing we should strive for.
I broadly agree with the approach to early stuttering described above, with the understanding that attention must also be paid to the preverbal stage. After all, much has already happened before a child exhibits stuttering symptoms.
Dear Adrie,
Thank you so much for sharing your thoughts.
We see a big advantage of having a stutter affirming approach with young children. For the younger sibling who not (yet) stutters, there already is a supportive environment. We think that helps the children you refer to.
All the best,
Joeri
Dear Joeri, Femke, and Tjitske,
Yes!! Yes, and yes again. Thank you for your article. Early therapy is so important for the very reasons you write about, in my view. I also believe that for those in group 2A, there may still be reactions to their stutter and/or may impact on them or their caregivers so early therapy can be helpful…..along with having a network of people who know more about and understand stuttering and help in reducing the stigma.
I have a lot of internal debate with myself about ‘Group 2b’ when I work with young children and their families. I suppose I had been taught that therapy (to reduce stuttering) can help this group, yet I’m embarrassed to admit that don’t know where this knowledge comes from. And so, I worry that I am neglectful of this group in the kind of therapy that I offer (which values and affirms stuttering and makes no attempt to reduce it). Your final paragraph offers me reassurance.
I’m guessing that when you speak of easing communicative pressure by (reducing questions, encouraging turn taking, etc), this is with the goal of making space for stuttering? I continue to have conversations with myself about the helpfulness of interaction strategies when their goal has been to reduce stuttering and to consider then how instead they can affirm stuttering. I see how some can support communication, give time and space for stuttering and welcome joyful connections with others…..and perhaps too then, reduce some of the associated struggle (if there is struggle)??
Thank you for sharing! It’s a joy to read.
Hi Nic!
Thanks so much for sharing your doubts! It really is a tough cookie to wrap your head around, isn’t it?
I totally agree with what Femke is saying. I think you should always help the child (and family) with struggle (behaviours), and never say: ‘you(r child) stutter(s), just accept it’. If the struggle is the struggle to not stutter (or stutter less), our plea for stutter affirming therapy is even more relevant. When the goal with parents is the fading out of stuttering (window of opportunity, etc) ánd you want to work on accepting stuttering to reduce the struggle… I think you will not get there. We all know this from our older clients.
The young child will notice that the parents want the stuttering gone, so the child will continue to try to achieve this. Therefor the starting point is the parents. Of course there might be a risk that the parents say they accept it, because they think you want to hear it. Interesting thing is, and this happened in a majority of cases: when we are a bit further in therapy, and communication is effortless and joyful, I sometimes see some minor things that could help get even a bit further. Most parents say at that point (while I thus suggest to continue) that they are happy with how it goes, nothing more is needed.
All the best!
Joeri
Dear Joeri,
Thanks for your reply. It makes such sense to me.
I think for the most part, I feel peace in the way that I work with families and little children. I think my doubt is just me trying to reconcile the way I work completely in my own head because I know from the older children and adults that I work with that living with stuttering can (for some), be hard. In my heart, I am true to the notion that stuttering is more than okay.
I too see the same picture further down the line in therapy that you mention – that caregivers (and the young people) are happy and need nothing more when communication is truly effortless and joyful!
Nic
Dear Nic,
Thank you for your detailed response and personal reflection. I think a lot of therapists recognize this internal debate you describe, at least we did ;). Therefore, we hope that this article serves as an invitation to continue this discussion with colleagues around the world.
The size of group 2b still remains unclear in our opinion. We were also trained with the idea that early intervention is important to reduce or stop stuttering. And for older children (>6 years or if the stuttering has existed for more than 2 years) the goals are focused on acceptance. But how can children and parents be guided properly and carefully in this 180-degree shift in goals? And to what extent is there, deep down, still a seed of stigma being planted? That is why we believe that the focus of early intervention should be on reducing and/or preventing the impact stuttering can have on quality of life, rather than on the stuttering itself.
Yes, that is what we think of: the goal of easing communicative pressure is to create space for stuttering and to help children learn enjoyable and effective communication. A side-effect might indeed be that there will be less struggle, if children experience at a very young age that there is truly space to speak with stuttering, no matter how long these moments of loss of control last.
Kind regards,
Femke
Dear Femke,
I wholeheartedly agree with you! I really value your thoughts and response.
I suppose what I didn’t clearly articulate in my original message was that because of the way that I view/value stuttering, and my commitment to a stuttering affirming approach from the outset of stuttering beginning, I feel a sense of guilt, doubt, worry about this group of children, because therapy to reduce stuttering is not aligned with my thinking. I find this hard. Nonetheless, my focus would only ever be reducing the impact of stuttering, fostering spontaneous and joyful communication with or without stuttering, and empowering our little ones to communicate authentically and freely.
Nic
Thanks for explaining this in more detail! That is so relatable… When parents (or colleagues) feel that you should do everything possible to reduce stuttering — ideally to 0% — it can feel as though you’re letting them down if you choose an approach that is truly stuttering affirming, as if you’re depriving the child of the chance for their stuttering to naturally fade away. However, we think; for some children, stuttering does fade, and for others, it doesn’t. For both groups we want to prevent the iceberg from growing and make sure we don’t contribute to the stuttering stigma ourselves.
Thank you Joeri, Femke, and Tjitske. You state that “there has -as far as we know- never been a study on harmful side effects of therapy.” Although I am not an academic researcher, my last book which came out in 2023 has gained respect of many who are. It’s called “VoiceS Unearthed: The Impact of Childhood Intervention on Those Who Continue to Stutter.” I agree, the aim for younger children should be to help parents nurture an environment of joyful communication, free and abundant speaking and effective communication. Parents can have a tremendous influence that can be far more impactful than the 1/2 hour a week a child may spend in traditional therapy. Thank you so much for your work and your efforts. This is where we need to go when it comes to treatment for young children and their families.
Thanks so much for your reply Dori. You are so right to point out your book, which is of great influence (we certainly are aware of it). We meant to say that most standardised programs have lots of research behind it. With main outcome measure of an SSI score. But -as far as we know- none of them looked at side effects. You are right, we could have expanded that ‘claim’ with your book. Thanks so much!
Joeri
Hi Joeri. Yes, the focus on SSI has been relentless! So grateful to hear about your work!!
Thank you for this insightful article. As a future SLP I want to provide my future clients with the most beneficial treatment I can. I love that you have rephrased the overall goal of therapy into something realistic and attainable for all young children who stutter. I also appreciate the idea of changing the language away from stuttering as a disorder and instead viewing it as a variation or difference in communication. I agree that intervention should focus on reducing pressure while communicating and reducing the impact of stuttering on the individual.
Hi Rayana, Thank you so much; and so great to hear your thoughts! Great to have you as an SLT in the future, keep up the good work!
Joeri
‘Reducing stress around stuttering as the first step’, that is indeed key and so very very important!
Does CESS (Certified European Stuttering Specialists) support and promote this new focus?
Hee Gijs! You’re welcome, thanks for reading and reacting! The three of us wrote this article from our expertise and experience in daily therapy-life. To give the reader a notion of what we are up to (work-wise) we tried to be as complete in our bios as we could. I’m (just) one of the board members of CESS (which is a certification organisation, we do not promote any therapy etc); if you’d like to know more: please drop the board an email through the contact form on the website.
All the best!
Joeri
Hello!
I loved reading this article about the research your team has done. Specifically, I enjoyed how you said the goal of therapy should be “to enjoy communication, speak freely, or communicate effectively”. As a future SLP, I love this approach to working with young children who stutter. This encourages communication, rather than cease communication due to fear, worry, or judgement. When working with children who stutter in the future, I hope to use a similar framework to best support my clients and their ability to communicate with the world around them!
Thank you so much, and great to hear you’re eager to work with this way of thinking!
“We make communication fun (again)” 🙂 – beautifully captures the essence of supporting both children and their families. I hope this idea can continue to inspire more therapists to shift the focus from fluency to confidence, joy, and authentic communication. Thank you for your work!
Joanna
Thanks Joanna! We hope that too 😉
Hi all
“it is crucial to give them -right from the first session- the strengths they need”. How I wish this would be the goal of all treatment: to give them the strengths they need. And the knowledge. And not just the child or the parents, but everyone around the child. The students, the teachers, the staff in the school restaurant, grandma, so that all learn what stuttering is and how to interact.
As a mother myself I know you are sad seeing your child struggle. But what if we could build up that child, making it strong enough to understand and to talk about it (I so love the booklet “I just stutter”, even if if the facts might be outdated). Giving it the tools to deal with bullies. Educating the people around the child. Talking about stuttering so the child knows it’s not something “wrong” and give space for all emotions around stuttering. Giving the child a voice to decide whether it wants to simply keep calm and stutter on with its friends who don’t care, or find a smörgåsbord of tools to make talking easier. What if the stuttering wasn’t the issue that needs to be treated, but society? What if acceptance wasn’t something PWS need to learn, but society?
All the years of hosting stutter camps for kids and young adults, listening to their stories, have taught me one thing: the no 1 things they want is to simply be accepted, whether that’s something they were born with (stuttering, red hair) or something they chose to (fashion, music).
So thank you for being the amazing team you are, enjoy camp DSL, and keep them talking.
Anita
Thanks so much Anita!
I like the relational model a lot: it’s about the interaction between the person and society. It’s not one or the other, since the person who stutters is also part of society.
Join us for Camp DSL someday. You’re more then welcome!
Fenke, Joeri and Tjitske, thank you so much for sharing this great piece of work! Keep on sharing and keep up the good work!
Manon
Thanks so much!!